Subscribe To MaysMicro


Wednesday, April 29, 2015
Measles in the Backyard
A new measles outbreak in New England! Check out this post on www.InfectiousNews.com
Saturday, April 25, 2015
Exploring Reusable Grocery Bags with the WGME News Team
Check out the full post on our upcoming news report at Infectious News
http://www.infectiousnews.com/#!Exploring-Reusable-Grocery-Bags-with-the-WGME-News-Team/cjds/553bb97f0cf23d01644f885e
http://www.infectiousnews.com/#!Exploring-Reusable-Grocery-Bags-with-the-WGME-News-Team/cjds/553bb97f0cf23d01644f885e
Tuesday, April 21, 2015
What Might Have Been: MMR Vaccines are not linked to Autism, and This News Infuriates Me.
What Might have Been can be found at our new site Infectious News
http://www.infectiousnews.com/#!MMR-Vaccines-are-not-linked-to-Autismand-This-News-Infuriates-Me/cjds/5536d8200cf2731334e2bbda
Thanks for reading!
http://www.infectiousnews.com/#!MMR-Vaccines-are-not-linked-to-Autismand-This-News-Infuriates-Me/cjds/5536d8200cf2731334e2bbda
Thanks for reading!
The Return of Bird Flu to the News
We have a new website! Please follow this link to see this piece:
http://www.infectiousnews.com/#!The-Return-of-Bird-Flu-to-the-News/cjds/5536883b0cf23d01643e2302
http://www.infectiousnews.com/#!The-Return-of-Bird-Flu-to-the-News/cjds/5536883b0cf23d01643e2302
Sunday, April 19, 2015
The Aftermath of Lyme Disease
(check this post out on our new site, Infectious News)
Every so often, a disease becomes shrouded in rumor and innuendo until it is difficult to parse out truth from fiction. People can take “pro” and “anti” stances, and the topic becomes unnecessarily charged. Anyone suffering from that disease can become either an involuntary “champion” or the subject of intense eye-rolling. This is clearly the case with Lyme disease, or more specifically, an ailment called “post-treatment Lyme syndrome” (NOTE: this is distinctly different from the widely circulated name “chronic Lyme disease”, which is a hotly contested and widely debated concept).
Every so often, a disease becomes shrouded in rumor and innuendo until it is difficult to parse out truth from fiction. People can take “pro” and “anti” stances, and the topic becomes unnecessarily charged. Anyone suffering from that disease can become either an involuntary “champion” or the subject of intense eye-rolling. This is clearly the case with Lyme disease, or more specifically, an ailment called “post-treatment Lyme syndrome” (NOTE: this is distinctly different from the widely circulated name “chronic Lyme disease”, which is a hotly contested and widely debated concept).
Most people who
become infected with Borrelia burgdorferi
following a bit from an infected tick will develop classic symptoms of Lyme
disease including a high fever, malaise, headache, painful joints, and in somewhere
between 60-80% of cases, a very distinctive rash. This rash is called erythema migrans, but is
more commonly known as a “bull's eye rash” for obvious reasons (see images below)! The rash is where a lot of the trouble comes
from. Most of us in the Northeast know
that a fever and a bull's eye rash means that one must get to the doctor for Lyme
treatment immediately. Patients presenting
this way are usually prescribed the appropriate antibiotic (doxycycline as a
standard) in a timely manner and almost always recover fully. Those
patients who are the 20-40% without the bullseye rash can run into trouble
getting a timely diagnosis and the appropriate treatment. This
is a problem.


B. burgdorferi
initially replicates very happily around the site of the tick bite, and then
eventually makes its way to the joints. Occasionally
it finds its way into the heart. Eventually
the bacteria invade the spinal cord and brain if left untreated. One could see where a timely diagnosis and treatment
would be critical, given that inflammation and damage done to joints, heart
muscle, and especially brain does not readily heal. Even if the bacteria are eliminated by
antibiotic therapy, the damage they generated tends to leave lasting
consequences. These can include joint
degeneration, arrhythmias and other cardiac complications, cognitive impairment,
hearing or vision loss, loss of motor coordination, possible psychiatric
effects, and above all, chronic pain.
Such ailments are life-altering, and should be taken as such.
The internet is likely both the best and worst thing that
could have happened for post-treatment Lyme syndrome. Patients suffering from chronic illness often
benefit from connecting with others in similar situations. On the other hand, there is space for
ambiguity in this case because some of its clinical presentations are not
visible and the mechanisms underlying the disease are still being discovered as
we speak. Ambiguity and the uncensored internet
are not necessarily a good combination, and are breeding grounds for zealots and charlatans (such as these from the "FDA" at FDA.com, not to be confused with the actual FDA at FDA.gov).
All manner of problems have become connected to “chronic Lyme disease”, often
with a complete and total lack of peer-reviewed evidence, such as this and this. This leads some to conclude that anyone with
post-Lyme complications is a malingerer, a drug seeker, a conspiracy theorist, or in need of a mental
health evaluation. As described above, this is not the case. That said, every claim made on the internet
cannot and should not be counted as fact.
In preparing this short piece I have spent quite a bit of time reading
the most recent peer-reviewed research, and was left feeling a bit overwhelmed
by the nuance of this disease. It is
extremely complex, and the design of each study coupled with its statistical methods
therefore become critical in evaluating the conclusions. I definitely feel that an hourly “Lymeology”
series is in order to tease some of these nuances apart. Sufficed to say that there is quite a bit of
complexity and much more work still needed to be done and published, and in
those situations, rumor and innuendo can take over. When they do, the entire topic becomes
nuclear and polarizing. Those who
suffer? The 10% of patients left with lasting
complications whose treatment is often a clinician’s best guess rather than an
established standard of care.
In closing, it’s just about tick season, and it is predictedto be a bad one. If you want to avoid a first-hand experience with this topic, it’s best to prevent infection in the first place. Here’s how.

Perspective of tick size, for your nightly checks (image: dhs.wisconsin.gov)
Sunday, April 12, 2015
Happy 60th, Polio Vaccine
April 12, 1955, 60 years ago today, a much celebrated medical breakthrough was announced. Before this breakthrough, those suffering from the disease it prevents could be left with partial paralysis, atrophied limbs, confinement to braces, wheelchairs, or iron lungs. That is a description of survivors, of course. Not everyone lived through polio. It was a disease that primarily affected children, though its most infamous patient was the longest-serving president in U.S. history. It most frequently struck in the warmer months, and as such, summer fevers always instilled a sense of dread in parents of small children. Was it a case of sniffles or the start of polio? Would their child recover, be left paralyzed, or die? If the first child recovered, would he spread it to his siblings? Would they recover? Terrifying.


Patients in "iron lungs"
(Photos: University of Pennsylvania [top]; Polio Canada [bottom])
The medical intervention was the first successful polio vaccine, developed by Dr. Jonas Salk. While the story of polio immunizations has something for everyone (really! There is competition, political scandal, jealousy, pettiness...a veritable soap opera), the aspect that is worth celebrating on this day is its inarguable success. This photo speaks volumes about how this breakthrough was received by families with small children:

Parents and children line up to receive Dr. Salk's vaccine and
ensure their protection from polio
That line stretched for blocks. At this stage of life and career I do not often have realizations about diseases that gut-punch me. Somehow, though, I never thought about the fact that in 1955 my own grandparents would have been standing in those lines, toting my mother and father, aunts and uncles. If you are in proximity to my age (35), that should give you pause. But for Jonas Salk, perhaps you would not be here. In our current global situation which paradoxically contains both voluntary vaccine exempters and outbreaks of polio from infrastructure-related vaccine lapses (most recently noted in Syria, Somalia, and South Sudan), we would do well to remember and celebrate April 12.

A grateful nation acknowledges the gift
Friday, April 10, 2015
New Reports of "the Next Tick-Borne Plague", Powassan Virus, are Getting Attention

(Photo: Getty Images)
A recent report about the detection of Powassan virus, described as "even worse than Lyme disease!", in southern Connecticut ticks has gotten a lot of attention. The report from the CT ag station by Anderson and Armstrong was not so surprising, though: Powassan has been detected in New England for many years. In fact, they reported it in 2012 as well. Another report by Nofchissey et al. showed that it has been infecting deer in Connecticut, New Hampshire, and Maine as far back as 1979. This Morbidity and Mortality Weekly Report review indicated human Powassan cases were reported in New Hampshire, Maine, and Massachusetts in 2013 (2014 numbers not yet published). So we see that Powassan has been "with us" for quite some time. Does this mean that I feel that this story is overblown? No, not at all. I am grateful to see the attention being paid to tickborne encephalitides, because frankly they are scary. Powassan and its nasty friends can cause encephalitis, or an inflammation of the brain. This is a terrible pathological state to be in. The mortality/fatality rate for encephalitis is quite high, but something that is not discussed as much is the morbidity, or rate of long-term health problems in survivors. It turns out that surviving encephalitis, in some instances, is no gift. Fortunately, the majority of persons infected with Powassan will have no symptoms of any kind, or will simply feel a bit under the weather for a few days. We may hear about a spike in cases this summer, but I suspect that will be due in part to the report from the ag station. As happened in Minnesota, exemplified by this letter to the editor of Emerging Infectious Diseases, surveillance went up, diagnosis was attempted more often, and thus it was found more frequently. The attention this brings is a good thing in another way: the intervention here is tick and insect protection. By more people undertaking it, there will be intrinsic protection against Lyme disease, Eastern equine encephalitis, west Nile virus, ehrlichiosis, rickettsiosis, La Crosse virus, and many others. I'll count that as a success!
Tuesday, March 31, 2015
About that Medieval MRSA Remedy...
Over the past 24 hours, I have seen approximately five million references to the following news story:
Anglo-Saxon Cow Bile and Garlic Potion Kills MRSA
Anglo-Saxon Cow Bile and Garlic Potion Kills MRSA

Ancient medicine cures all!! We're saved from MRSA! This seems very exciting! Something that kills the indestructible 'superbug' MRSA, or methicillin-resistant Staphylococcus aureus, is desperately needed from setting medicine back 100 years. Now we have the answer! Er...maybe not.
Here's the thing - this finding does not surprise me in the least. Garlic, onions, and most certainly bile have all been shown to inhibit bacterial growth in a laboratory. I do not find this report particularly astounding at all. For topical use on wound infections, it could be a helpful solution. However, topical infections do not usually kill people. Septic, visceral, lung, and central nervous system infections do. In those cases those pesky factors like toxicity (is it poisonous?) and pharmacology (is it digested? Is it absorbed into the bloodstream? Can it cross the blood-brain barrier?) become important. In deference to those obnoxious and weedy details, I present the following (non-exhaustive) list of things that will kill MRSA:
- Hydrochloric Acid
- Arsenic
- Ionizing Radiation
- Bleach
- Fire
- 200 proof (100%) ethanol, isopropanol, or methanol
- Cyanide
- Volcanoes
- Chlorhexidine
- Iodine
- Sulfuric Acid
- Glass beads
- Honey
- Sodium hydroxide
- Formaldehyde
- Neosporin (really!)
- Autoclaving
- French press
- Freezing it at -80 celsius and then rapidly thawing it at 60 celsius a few consecutive times
- Nail polish remover
My point here is to take this very cool and fun story with a grain (boulder, whatever) of salt. Something that kills bacteria does not necessarily make a great clinical antibiotic. In any event, prescribing "fire" for patients seems like there would be a lot of forms involved.
Sunday, March 29, 2015
Foreshadows from the Science Fair
Two important things will happen this April (though I concede only one of them is important outside of our household): my eldest son will participate in his first science fair, and the anniversary of the Reagan Administration's first public acknowledgement of HIV and AIDS will occur. Those two things seem completely unrelated, but in my world they are very tightly linked. My elementary school science fair project was originally titled "Germs", until my mother corrected me on the term and had me title it "Disease-Causing Microbes" (thanks, Mom). I had always found disease interesting, and the science fair seemed like the place to act on it. My mother, a nurse practitioner with an MPH, was a willing resource and shared many of her books. I began making a poster with lists of the different types of "germs" (er, disease-causing microbes). While I was working on a column about viruses, she told me that I had to put "AIDS". I replied that it wasn't in the books and she, her voice strained, agreed. "But it will be someday, and it's important that you add it."

In hindsight, I get it. I get the strain in her voice, and her insistence that this newfangled AIDS thing was a big deal. I was a little girl, and I didn't know that people were dying of a disease that the US government was stubbornly refusing to acknowledge largely because of whom it tended to affect. If I had known, I wouldn't have understood why. In the years since, the US government and US-based foundations have poured billions of dollars into the science, diagnosis, treatment, and prevention of this disease. Not bad for 31 years of work. Not bad at all.
As for science fairs? Sometimes they foreshadow things. If history repeats itself, my son will be a professor writing a paleontology blog (or whatever the modern equivalent is) at 11:30 PM someday. Sometimes science fairs give the intellectual kid a chance to be rewarded as such. Or at the very least, they create yet another reason for my boy to talk about dinosaurs.
Saturday, March 28, 2015
Talking About Vaccines: Maybe We've Been Doing it Wrong

(Image: Coursera, "Epidemics- the Dynamics of Infectious Disease")
Recently I have been working on a piece for the Bangor Daily News about pending legislation in Maine that would make vaccine opt-outs and exemptions more difficult to acquire. This is an important topic up here, since our immunization rates fall below herd immunity threshold. Translation: unvaccinated persons are officially at elevated risk for contracting vaccine-preventable diseases. This not only means the medically exempt; it means kids who had been exempted voluntarily, and most tragically of all, all infants up to one year of age. As such, members of the state legislature have introduced a bill to address this problem and restore the state of Maine to herd immunity levels in defense of all infants and the medically fragile. Makes sense to me.
I have been having trouble writing this piece, because every time I finish it, I hate it. It sounds like every clinical or scientific defense of vaccinations I've ever read (those snarky ones on BuzzFeed and HuffPo, or this wonderful piece in Grounded Parents notwithstanding). Why should this piece be any different from the others, where we try and repeatedly fail to sway hearts and minds into protecting children? How the heck do we lose this argument so frequently? It's baffling! This seemed well outside my expertise, so I started talking to some colleagues who are experts in neurosciences. Paydirt.
Of the phenomena discussed, one has given me something reasonable to try with this article. Apparently somewhere deep in the limbic system, our brains are conditioned to believe things as true based not on how much sense it makes, but on how many times we've heard it. Reading up on this a bit more, I found a paper that discussed this idea with regard to vaccine policy. The upshot of my exercise is this: by systematically debunking vaccine myths, we keep repeating them. The context is irrelevant to that very primal part of our brains. We keep repeating them. A great example I can think of here would be the "birther" nonsense about Barack Obama. No matter how many ways his birth in the state of Hawaii has been documented, verified, and everything else, a disturbingly high number of people still believe he was born outside the United States. Instead of saying "in response to suspicions he was born in Kenya, blah blah blah", a more effective presentation would have been "President Obama was born in Honolulu, as documented here." The second statement does not repeat the myth, and the first does.
I am going to start my BDN piece from scratch. I am further going to reconstruct my course materials for the med students on how to talk with patients about vaccines. "In the state of Maine, a 6-week-old infant is at risk for contracting whooping cough due to low immunizations rates. This has a high rate of death, and an almost universal chance of leaving surviving infants with permanent damage to their respiratory tract. A critical way to address this is to ensure that everyone in the household has received a safe and effective TDaP vaccine" would hopefully be a good place to start!
Tuesday, March 24, 2015
What Doesn't Kill You...
...may leave you permanently disfigured, disabled, and shunned, if we're speaking about infections. In particular this is true of a group of ailments known as "neglected tropical diseases", or NTDs. These are infections that disproportionately (and in most cases exclusively!) affect those in developing countries across the tropics. We may be tempted to think that because they do not leave millions of deaths in their wake, they are not an important health topic. This could not be further from the truth. Take infection with the parasite Onchocerca volvulus, for example. This worm infects the eye, and causes terrible scarring of the cornea as the immune system tries desperately to kill off the parasite. Never mind the maddening feeling of a worm twitching and rolling in one's eye; the most impactful outcome of this disease is the corneal scarring. Patients are left blind, hence the common name for the infection of "river blindness". Those affected are often left unable to work, hunt, farm, and otherwise maintain their economic security.

A young South Sudanese woman with river blindness due to Onchocerca volvulus (Photo from http://therefugeeroad.blogspot.com/ )
Perhaps more infamous among these diseases is elephantiasis (or lymphatic filariasis, clinically speaking). This is caused by a few different species of parasitic worms including Wuchereria bancrofti and Brugia malayi, and is characterized by intense swelling of individual limbs, causing them to resemble the limbs of elephants. The limbs are swollen with lymph fluid and adult worms. If a patient is able to access anti-parasitic medications such as ivermectin or albendazole, this will only keep them from transmitting the disease to others. It will not cure them. If every living worm was killed, the disfigured limb would remain. Similarly, the stigma would remain. Though elephantiasis is transmitted by a bite from an infected mosquito, the perception of patients as unclean is widespread. Affected persons are often unable to find a willing employer even if they are physically able to work. Some are shunned by their families. This disease may not kill, but to pretend it is therefore unimportant is a fallacy.

An elephantiasis patient in Bhutan (Photo: Mark Brazinski)
How can one help solve this problem? Prevention of infection is key. This means widespread access to medication or more ideally the development of preventative vaccines. Since these will by definition be unprofitable endeavors, research studies to discover and develop them are often funded by Federal governments, international agencies, or charitable foundations such as those run by Jimmy Carter and Bill and Melinda Gates. In addition to politically or financially supporting research, there are other ways to address those already infected. A growing number of companies seek out NTD patients as employees as part of their business models. One of my favorites is Global Girlfriend, which employs women as artisans to hand-make clothes, jewelery, and accessories and sell them worldwide via the internet. Most touching, every order includes the story of the woman who made the product. My particular favorite is my Congo Solidarity Skirt ("river"): it was made by a woman who lost the use of her leg due to polio, and was abandoned by her husband. She now has an income and a home. There are many ways to have an impact on these non-killing, life-shattering diseases. Please remember them.
Wednesday, March 18, 2015
TB is Trending on Facebook!!
And Let's not Forget What we Just Learned
Several weeks ago a high school student in Kansas was diagnosed with active tuberculosis, a disease characterized by cough, fever, night sweats, and wasting. Active TB patients are capable of transmitting the infection to others, but those others typically do not become sick right away. The TB bacteria infect their lungs in a dormant state, termed latent infection. These individuals are not contagious; the bacteria are sequestered in their lungs, and they are not coughing to facilitate its transmission.

TB bacteria sequestration in lungs during latent infection
L. Ramakrishnan, Nature Reviews Immunology 12: 352-366, 2012
L. Ramakrishnan, Nature Reviews Immunology 12: 352-366, 2012
As it turns out, the first student has infected 27 others, who are now in the latent stage of the disease. Those students are not contagious. All 28 persons are currently undergoing antibiotic treatment, and are expected to recover fully without infecting anyone else. How frightening is it that there are 28 tuberculosis patients in Kansas? It is actually quite a normal level. We do not tend to hear about it, but TB is not spectacularly unusual in the least.
As we just learned with Ebola, assessment of risk to others is well understood. Nothing to worry about here.
A New Ebola Case in the US Illustrates Our Collective Learning
A clinician working with Partners in Health was evacuated to the US from Sierra Leone after developing Ebola virus disease. The patient is currently being treated at the National Institutes of Health, and is at present in critical condition. Early in infection this clinician was treated/attended by twelve of his or her colleagues resulting in their exposure to Ebola, and they were similarly evacuated to the US and remain in quarantine (note, not isolation) in Nebraska, Maryland, and Atlanta. One contact in Omaha showed clinical signs Monday and was promptly isolated; however, that patient has since recovered and has thus far tested negative for Ebola.

A PIH Clinician treats an Ebola patient (photo courtesy of Partners in Health)
There is a subtle, unspoken victory here that warrants a celebration of sorts. I looked this morning on CNN for an update on this patient's condition, and could not find one. Similarly, ABC News had not written about this case for 3 days. In October, this would not have been the case. In October, there were loud cries for the blocking of Ebola treatment of American citizens in the US. Among my least favorite descriptors - "those people" - was frequently shouted. No one is shouting now. No one is being vilified. No one doubts that this patient, who can only be described as selfless and heroic for how s/he became infected, deserves to come home and receive medical care. I take this to mean that we as a society have learned. We have come to realize that no one was being lied to; no one was promising safety where there was imminent danger. I take it also to me that we as a profession are a small step closer to regaining some trust.
May you be well soon, NIH Patient. Thank you for your service.
Tuesday, March 10, 2015
One is too Many
Though it has faded from the headlines to some extent, new measles cases continue to be diagnosed in the US following a large, multi-state outbreak of the vaccine-preventable disease. Patients were initially exposed following visits to Disneyland, and satellite cases appeared across the country. What has not been discussed much is that satellite cases have also appeared in other countries that were exposed in California. The World Health Organization report "Measles-The Americas 2014-2015" also describes a fatal case in Brasil.

Pushback against criticism of parents who choose not to vaccinate their children for nonmedical reasons has included arguments that "measles is not that bad a disease", and "only 1 or 2 in 1000 patients die" (called out in this excellent piece in Science Based Medicine). Excuse me, can you repeat that? "Only 1 or 2 in 1000 die"? One in 10, 1 in 1000, 1 in 1000000...if the "one" is someone you love, it doesn't matter one damn bit how many other people were left alive. This has to particularly sting if you chose not to vaccinate your child. This is an exceptionally cruel reality when your child is unable to be vaccinated (often due to age in the case of measles). In a circumstance such as measles where there is a safe, cheap, and easy way to prevent it? One is way, way too many.
Courtesy of the Centers for Disease Control and Prevention
Monday, March 9, 2015
Victory in Liberia
Late last week the last known Ebola patient in the country of Liberia was discharged from the hospital. This represents a number of victories, both large and small. Beginning with first principles, Beatrice Yardolo left the hospital alive and well. Things will never be the same -three of her children lost their fight with Ebola- but she recovered. Last year at this time, when workers for MSF were sounding an alarm that went unnoticed for several more months, a patient leaving the hospital in anything other than a body bag was something to celebrate.

'Someday' is not in sight, however. While Nigeria, Mali, Senegal, Spain, and the United States are now considered free of Ebola and there are no known active cases in Liberia at the moment, there is still a lot of work left to do in Sierra Leone and Guinea. Both have see cases begin to resurge a bit after a lengthy decline. But we as scientists have learned a lot in a very short time about Ebola, and I am cautiously optimistic.
For Liberia, the work of fighting the epidemic is taking a backseat to the next challenge. For Liberia, it is time to rebuild.

Beatrice Yardolo begins the rest of her life (Photo Abbas Dulleh, AP)
This epidemic was so different from previous outbreaks in many ways. The sheer size and scale of it was unprecedented. The circulation in major cities was a new and terrifying feature. The departure of Ebola from the African continent resulting in spread between humans had never happened before. The epidemic has sustained for over a year. Many, myself included, suspected that Ebola would become endemic in West Africa. In other words, it would become entrenched enough that transmission would just go on continuously between humans, and the epidemic would never officially end. The discharge of Ms. Yardolo signals that we were most likely wrong, and the epidemic will end someday. That is outstanding news. 'Someday' is not in sight, however. While Nigeria, Mali, Senegal, Spain, and the United States are now considered free of Ebola and there are no known active cases in Liberia at the moment, there is still a lot of work left to do in Sierra Leone and Guinea. Both have see cases begin to resurge a bit after a lengthy decline. But we as scientists have learned a lot in a very short time about Ebola, and I am cautiously optimistic.
For Liberia, the work of fighting the epidemic is taking a backseat to the next challenge. For Liberia, it is time to rebuild.
Friday, February 27, 2015
Dr. Wakefield Goes to Oregon...or Not.
This week, I was astounded to read that Dr. Andrew Wakefield, he of the thoroughly debunked "vaccines cause autism" fame, had been called to testify before the Oregon State Legislature. The bill in question would ban parents from requesting non-medical vaccination exemptions, and Wakefield was called as an expert consultant presumably in support of the dissenting position. Except that he will not be allowed to testify.

Courtesy of We Love GMOs and Vaccines
Though alternative explanations were given, I'm going to (perhaps cynically) agree with my colleagues at We Love GMOs and Vaccines: they realized who -and what- Wakefield is, and declined further interaction. Well spotted, State of Oregon.
Monday, February 2, 2015
It Turns Out that Calling People Idiots is Ineffective
A friend of mine recently suggested that perhaps humor was a good way to do a little scientific education and outreach. Lecturing is too "professorial" (perhaps not unexpected from the likes of me, though); presenting quick nuggets of data appears ineffective. Making people laugh while educating? That could work. Jon Stewart's viewers routinely score best on random current events polls, so maybe there's something to it. I was thus excited to see that The New Yorker published a comic about the recent measles outbreak

Courtesy of The New Yorker
I'm sure you could all guess my opinion of parents who eschew vaccines. However, I think it far more important that children do not get sick. This? This will not change the mind of anyone on the fence. This is why we Northeasterners are reputed as being rude. Did I do a spit-take laugh upon reading it? Maybe. But it doesn't help. Opportunity missed, guys: you could have cracked people up AND changed minds with a different approach. No ever changed anyone's mind by calling them an idiot. You would think The New Yorker would be aware of that. I mean, what are you guys? A bunch of... never mind.
Wednesday, January 28, 2015
The Price of Willful Ignorance
For the second time in as many years, the United States has an active measles outbreak. This is inarguably due to elective omission of childhood vaccines. While the national US rates for all required immunizations remains within the bounds of "herd immunity", this is misleading. There are large pockets within the country where vaccination rates have dipped below this level, and unvaccinated children are at risk for contracting vaccine-preventable diseases. I am painfully aware of this; you see, I live in one. More importantly, my young sons live in one. The oldest is school-aged, and he is healthy enough to be fully vaccinated. The youngest is 16 months. He has had a single measles-mumps-rubella (MMR) vaccine due to his age. He will not be fully protected for another few months. Last fall, he was an infant with no immunity of his own to measles. We live in the Northeast, and the region had a measles outbreak. Someone else's poor choices cost easily have cost my son his health, his hearing, his eyesight, or his life. The unfairness of that cannot be understated. I am grateful that our pediatrician refuses to see unvaccinated patients, eliminating the possibility of my baby contracting it in the waiting room.
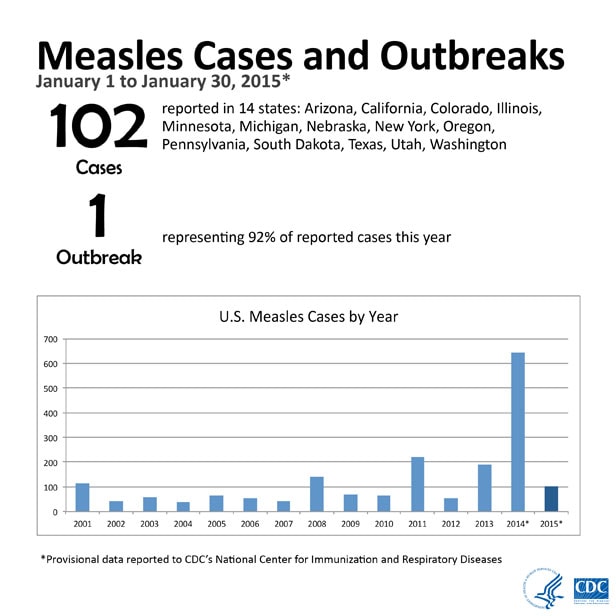
U.S. Centers for Disease Control and Prevention
I was lucky. Many families in Southern California are not. A few weeks back, an as-yet-unknown person went to Disneyland while infected with measles. This single patient infected additional individuals, most of whom were unvaccinated. Many of these were elective omissions, but some were not. Some patients were not vaccinated because they were infants who are too young. There have now been multiple secondary cases, meaning that patients who contracted the disease at Disneyland are spreading it in their communities. This is easily possible: some parts of Southern California have vaccination rates lower than South Sudan.
This is not only absurd. It's grossly unfair. Elective omission of vaccines (in other words, refusing them for nonmedical reasons) is not justifiable. They are among the safest and most effective medical interventions created to date. Despite this, many people will not vaccinate their children (against medical advice) because of rampant fear-mongering by persons without the background to make such judgements. When misconceptions are challenged, these folks are not persuaded. Many simply will not listen to reason. In fact, a recent study showed that these beliefs become more entrenched, not less, when their holders are presented with scientific evidence. This is willful ignorance, and it's dangerous.
It is tragic enough that willful ignorance by parents endangers their own children. When it endangers the health and lives of other children, I suggest it is well past time to stop enabling this nonsense. I am certain that Jennifer Simon, whose infant daughter is under a 28-day quarantine due to exposure to measles at a pediatrician's office, would agree. Similarly, I am sure the same is true of Katie Van Tornhout. Her precious daughter Callie died of pertussis when she was too young to be vaccinated: the very definition of an avoidable tragedy. We can do better than this.
Subscribe to:
Posts (Atom)